
Schaeffer Center White Paper Series | DOI: https://doi.org/10.25549/FBEW-6Z03
Key Takeaways
- Long-term or heavy use of cannabis—in particular, high-potency manufactured cannabis products—is associated with negative health outcomes, including psychosis, cannabis hyperemesis and addiction.
- Vermont and Connecticut are the only states that cap potency of THC on most types of cannabis products sold, despite this being a useful tool to prevent harmful consumption.
- Assuming a standardized dose of 10 milligrams of THC for average-potency cannabis products, all states allow purchases exceeding 500 doses. Current sales restrictions do not promote moderation in use.
- Taxes based on potency, rather than price or weight, do a better job of incentivizing moderate THC consumption.
- A single, federal, seed-to-sale tracking system will assist with enforcement of all policies and aid in public health research, particularly given the restrictions in place on scientific inquiry of these products.
A press release covering this white paper’s findings is available here.
Abstract
Millions of Americans use cannabis in moderation each month without any problems. However, evidence is mounting of harmful physical and mental health effects associated with heavy or long-term regular cannabis use. At the same time, existing legal markets in the United States are making high-potency cannabis products available to adult consumers. Recent international recommendations suggest that governments adopt market regulations that promote responsible use. Federal policymakers in the U.S. are debating liberalizing cannabis policy and looking to states and nations with existing recreational cannabis laws as examples. Amid this debate, it is important to examine the extent to which regulations within various jurisdictions promote responsible use and protect public health. We review elements of cannabis legalization policies across U.S. states, Canada and Uruguay that research suggests could be important for promoting responsible use. Specific policy areas considered include: capping the amount of delta-9-tetrahydrocannabinol (THC) in all products, instituting sales limits, taxing cannabis based on potency of THC and implementing seed-to-sale tracking systems. We find that current regulations of legal cannabis markets are weaker in the U.S. compared to Canada and Uruguay in terms of preventing harmful use across these dimensions. Federal policymakers should understand the strengths and limitations of existing U.S. state policies and consider public health regulations being adopted abroad when developing federal cannabis regulations.
Introduction
Since the Controlled Substances Act (CSA) of 1970, cannabis has retained its federal status as a Schedule I drug, contending that it has (1) a high potential for abuse, (2) no currently accepted medical use in the United States and (3) lack of accepted safety for use under medical supervision. Although federal law prohibits possession and distribution of cannabis in the U.S. (except for research purposes), vast changes in state laws and policies have occurred over the past two decades. As of May 2022, 19 states and the District of Columbia have legalized adult use or “recreational” cannabis markets. Another 18 states allow use of cannabis containing more than trace amounts of delta-9-tetrahydrocannabinol (THC), the main psychoactive ingredient in cannabis, for medicinal purposes; 10 other states allow only low THC (i.e., ≤ 0.3%) to be sold for medicinal purposes. Public support for legalization of adult use cannabis is at an all-time high of nearly 70%.1
In December 2020, the U.S. House of Representatives passed a landmark vote in favor of decriminalizing cannabis through the Marijuana Opportunity Reinvestment, and Expungement (MORE) Act with a slightly revised version passing the House floor again in April 2022.2 Senators Cory Booker (D-NJ), Ron Wyden (D-OR) and Chuck Schumer (D-NY) are expected to introduce a final draft of a similar proposal, the Cannabis Administration and Opportunity Act (CAOA), in August 2022, after soliciting public comments on a discussion draft in July 2021.3 As federal policymakers engage in more serious debates of the benefits of liberalizing cannabis policy, it is important to consider some key lessons learned thus far from experiments with recreational cannabis laws in U.S. states and abroad.
The statutory language of enacted state laws and proposed federal changes have largely focused on the goals of raising tax revenue, investing in communities most harmed by drug prohibition, eliminating the illegal market for cannabis and reforming the criminal justice system, specifically through expungement of prior offenses. These are important goals to consider when seeking to redefine cannabis policy given the significant harms and costs prohibition imposes on communities of color. Serious consideration also needs to be given to public health objectives and the value of a regulatory environment that promotes responsible use. The adult-use laws passed thus far in U.S. states have placed relatively little emphasis on public health objectives associated with promotion of responsible use. While preventing impaired driving and limiting youth access are generally mentioned in many states’ legislation, many states have failed to allocate adequate resources to implement appropriate technological changes and compliance checks to ensure these objectives are met.4,5 Furthermore, efforts to enact policies to disincentivize high-potency cannabis use (e.g., capping THC for all products, including flower), have repeatedly failed in five states despite clear public health harm from a rising number of unintentional poisonings.5,6,7
Policymakers should keep in mind two important points about the research to date when developing cannabis legislation. First, the lack of decades-long scientific evidence on the harms from excessive cannabis use is not indicative of cannabis safety, but rather an artifact of prohibition, which also restricts scientific investigation into the harms of different gradations of use. Just like other intoxicants, there is a dose-response relationship between use of particular cannabinoids and harm.8,9,10 Understanding dose-response relationships requires measurement of the precise amounts of specific cannabinoids being consumed and in what fashion, but actual measurement of cannabis use in data has been limited due to prohibition.11 Second, the THC levels in cannabis products evaluated in clinical studies provided by the National Institutes of Health are much lower than that available in dispensaries.12
This white paper describes why public health goals related to moderating consumption should be further considered and integrated into proposals to legalize cannabis federally. Cannabis legalization policies can minimize threats to public health while achieving social justice, equity and economic goals, but this requires the regulatory environment to prioritize the promotion of moderate, not excessive, use.
Early Evidence of the Impacts of Legalization on Potency, Prices and Public Health
Though few rigorous evaluations exist, early evidence from the U.S. demonstrates clearly that cannabis policy legalization is associated with (1) an increase in the potency of cannabis products available in the U.S. legal market;13,14,15 (2) a decline in the average price per gram and per dose of THC;15,16 (3) an increase in frequency of use, heavy use and prevalence of cannabis use disorder among adults, including among pregnant women;17,18,19,20,21,22 (4) a rise in pediatric and youth cannabis-related emergency department visits;23,24,25 and (5) a rise in cannabis-involved impaired driving.26,27,28,29 These observed changes in the U.S. market are due in part to the content of state regulations pertaining to both medical and recreational cannabis markets, as similar observations have not been reported to the same degree in other medicalized and legalized countries.30,31 One possible explanation is that specific elements of the regulations can influence the potency of products available on the market and hence implications for excessive use and public health harms.
Several challenges limit our ability to study the overall health impacts of cannabis use, and the effects of policy on these impacts, to the same degree that we have studied alcohol and tobacco. These include the lack of precise data on cannabis involvement (e.g., measuring recency of use versus use at time of the health event) and on the amount actually used and absorbed into the bloodstream; inability to isolate impacts of the use of cannabis versus other substances (tobacco, alcohol or other drugs); the variety of modes of administration, which can differentially impact absorption and impairment; and the lack of a standardized dose or measure of cannabis use within these products.32,33 Some of these challenges are unique to cannabis, while others also impact research on alcohol, tobacco and other intoxicants. Even with these scientific challenges, there is evidence of both therapeutic benefits associated with medical use and adverse health effects associated with nonmedical use, particularly among vulnerable populations.34 This paper is focused on identifying regulatory strategies that mitigate the negative health consequences of cannabis use while retaining availability of a high-quality, legal product.
Strong research evidence links long-term or heavy use of cannabis with impaired short-term memory and motor coordination (e.g., driving skills); increased risk of cannabis use disorder; impaired cognitive function; altered brain development; increased risks of anxiety, depression and psychosis in certain populations; and lower educational attainment.10,18,35,36 For many of these outcomes, it is difficult to tease out correlation from causal links, but associations have been documented across contexts, time periods and populations. Moreover, associations are larger in groups exposed to greater doses of THC. Adolescents are especially susceptible to the adverse effects of cannabis since their brains are still undergoing neurobiological maturation.37
Recent studies also point to a rise in negative health effects specifically associated with manufactured cannabis products, such as edibles, concentrates and liquids that can be vaporized.7,38,39 These products, which are typically higher in THC compared to flower, may be especially risky for inexperienced and vulnerable users.40 For example, in Canada, rates of cannabis-related emergency department visits and hospitalizations among children increased after edibles were introduced in the legal market.39 In states like Colorado where legal nonmedical cannabis markets have operated for almost a decade, there has been a rise in the number of cannabis-related emergency room visits due to acute psychiatric symptoms and cyclical vomiting.41,42
Policy Tools May Be Effective At Preventing Harmful Use of Cannabis
Testing of all cannabis products—when consistent, systematic and conducted by financially independent facilities—as well as regulations guiding the manufacturing and processing of edibles, concentrates and liquids are important preliminary steps to any public health agenda for establishing legal cannabis supply regimes. Indeed, many U.S. states have become increasingly aware of and taken steps toward implementing these regulations, as well as testing the integrity of these processes and procedures. At least four additional policy tools merit similar attention or consideration: (1) capping potency by limiting THC, (2) instituting sales limits based on potency and total THC purchased across products, (3) designing a tax structure based on potency of products and (4) implementing seed-to-sale data-tracking systems and compliance checks in a manner that enables regulation of products, testing sites, distributors and retailers. We focus on these tools because of their feasibility and potential effectiveness if implemented at the federal level. For each policy tool, we detail how it may prevent harmful or excessive use, describe how it is currently used (or not used) in state laws and federal proposals, and provide examples of how it is implemented in other countries.
1. Capping Potency by Limiting THC
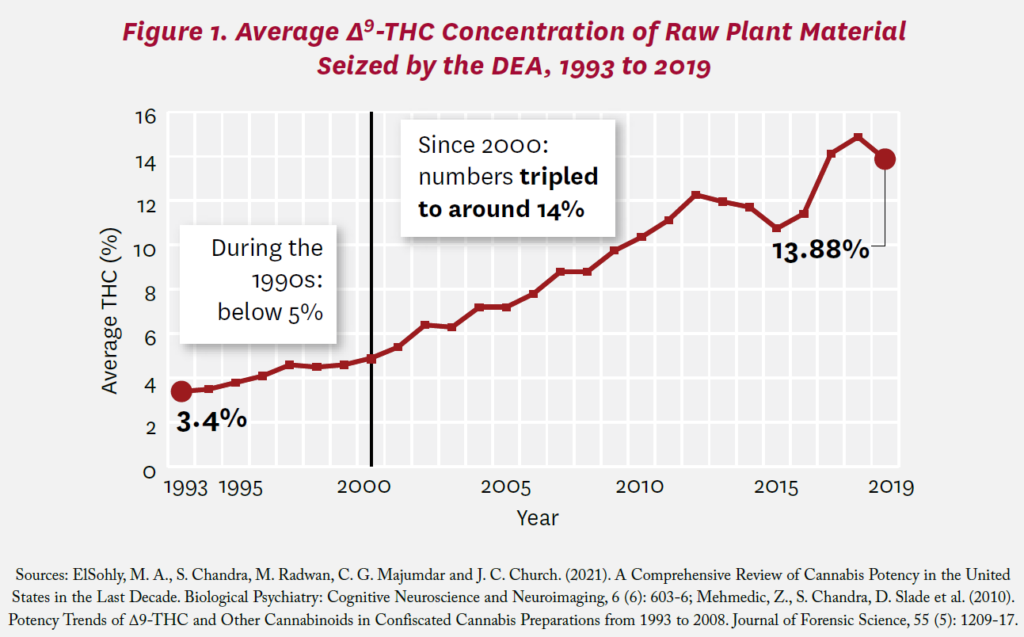
For decades, the University of Mississippi has been monitoring the level of different cannabinoids, including THC, contained in cannabis plants seized by the Drug Enforcement Administration (DEA). Figure 1 shows the trend in average THC from these samples over the past three decades. During the 1990s, the average THC reported in cannabis plants seized by the DEA was low, below 5%.43,44 Since 2000, the average THC in seized cannabis plants has tripled, to around 14%, slightly below the average THC levels found in dried flower in U.S. recreational markets, which ranges from 15% to 21% THC.15,16,40,45
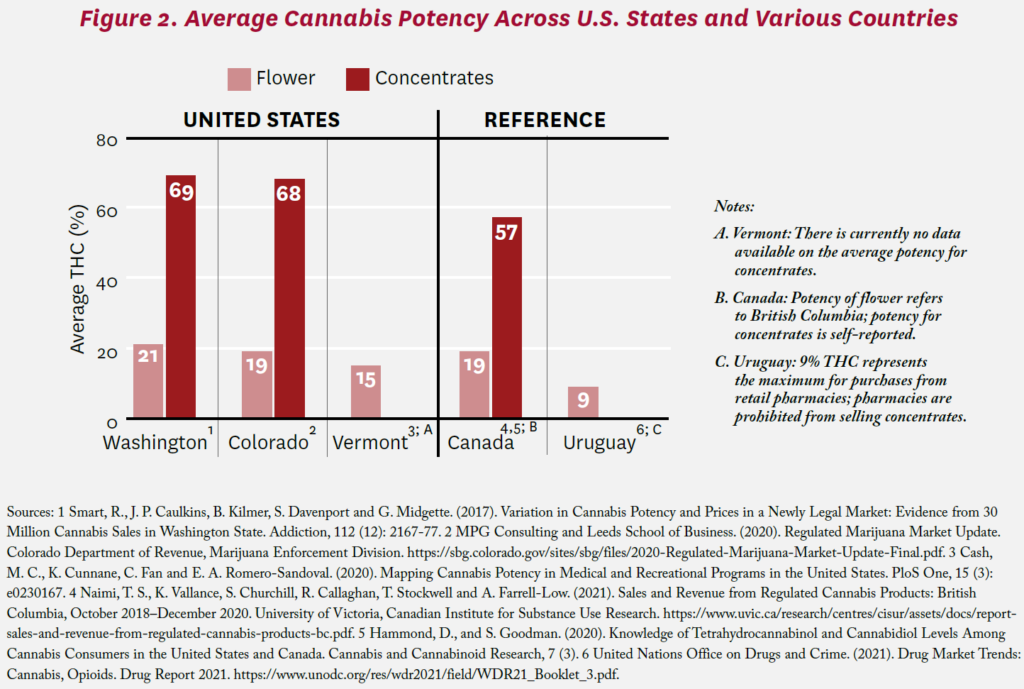
Innovation in the legal medical and adult-use cannabis markets has not just led to higher potency plants; it has also led to a proliferation of new THC-infused products, including edibles, concentrates and extracts, with average potencies far exceeding that of the plant itself. The average THC levels in concentrates and extracts are above 60%.40 Evidence from sales in legal markets shows that these high-potency products are becoming increasingly popular. During the first two years of legal operations in Washington, the market share for extracts for inhalation increased by 145%—from 8.6% in October 2014 to 21.2% in September 2016.15
In Oregon, sales of extracts and concentrates immediately jumped when recreational stores opened in October 2016, averaging 26% of total market sales each month between October 2016 and November 2018, the last month observed in the study.13 Survey evidence similarly reports a rise in use of these high-potency products, particularly among young adults and youth.46,47,48
To moderate use of cannabis and prevent adverse health effects associated with high-potency products, policymakers may consider capping potency for all products, including edibles, concentrates, extracts and flower, by setting a limit on the percentage or total amount of THC in a given product sold in the U.S. States would be allowed to set their own stricter limits. Potency caps are generally only considered for edibles in the U.S., although a few states also cap some concentrates. Of the 19 states and D.C. that have legalized nonmedical cannabis use by adults, Vermont and Connecticut are the only states with a potency cap on both flower and concentrates. Both states limit the percentage of THC to 30% in flower and 60% in solid concentrates sold.49,50 Both states, however, exclude prepackaged vape pens or cartridges from these potency limits. Throughout 2021, policymakers in other states, including Colorado, Washington, Montana, Massachusetts and Florida, introduced or drafted bills to similarly limit THC levels.51 These bills have either failed or been shelved until the following legislative session, primarily due to resistance from cannabis businesses and industry proponent groups, arguing that potency caps on the legal market will impact a large proportion of products and lead to diversion to the illegal, unregulated market.52,53,54 The inability of state policymakers to institute potency caps in markets that are already operating highlights the importance for federal proposals to include this policy at the onset of potential legalization.
THC potency caps on flower and other products are far from novel in other jurisdictions that have legalized cannabis for recreational use. Both Uruguay and Canada have adopted caps on potency for some products. In Uruguay, the maximum THC content across all products sold in pharmacies was initially set at 2% in 2013 and later increased to 9% in 2017. Extracts and edibles are prohibited, and only five companies are authorized to produce and distribute nonmedical cannabis.55 In comparison, the average potency is higher within Uruguay’s cannabis social clubs and home growers, where no potency limit exists, suggesting the potential effectiveness of this policy tool.56 Further, Uruguay’s cannabis regulatory agency (Instituto de Regulación y Control del Cannabis) estimates that the legal market accounts for over 50% of the country’s total cannabis users, indicating that the legal market has displaced a sizable portion of the illegal market even with strict federal regulations.57 In Canada, the maximum THC content is 10 mg/package for edibles, 10 mg/unit or dispensed dose for ingested extracts, with a maximum number of 1,000 mg per package of either an ingested or inhaled extract, and 1,000 mg/package for topicals.58 The potency of flower material is not officially capped. The most recent data show the average THC potency for flower in British Columbia’s legal market is 19%, comparable to that sold in the U.S., but higher than that reported for Canada overall.59,60 This suggests that the average potency of cannabis flower may be on the rise in Canada. Figure 2 illustrates the variation in average THC of various products across jurisdictions and product type. Experiences in Uruguay and Canada suggest that limiting potency may be a viable option for policymakers to reduce the availability, and hence the consumption, of high-potency products.
Finally, while capping THC levels offers a promising policy tool for limiting consumption of high-potency cannabis products, consideration must also be given to newly emerging products that contain natural or synthetic THC isomers such as delta-8 or delta-10 THC, or THC analogues such as THC-O-acetate, which is created from hemp, a plant that comes from the same family as cannabis but has been federally legal to produce since the 2018 Farm Bill.61 In a six-month period, from December 2020 to July 2021, the U.S. Food and Drug Administration (FDA) received 14 reports of patients admitted to the emergency room due to adverse effects from ingesting delta-8 THC food products.62 Over 600 exposure cases have also been reported to national poison control centers.62 THC-O acetate is known to be three times more potent than delta-9 THC and may have hallucinatory effects, raising additional public health concerns.63,64 These derivatives, which have not been tested or regulated in the U.S., demonstrate the ease with which the existing cannabis industry, keen on developing a regular consumer base, will innovate to attract new users. Some states, such as North Dakota and Michigan, have started to take legislative action by redefining THC to include all isomers and analogues under the same regulations.63,64 While it is unclear the extent to which such actions will be effective, this evolution highlights the need to think carefully about legal cannabis in terms of both current cannabinoids of interest as well as innovative derivatives we have yet to understand.
2. Instituting Potency-Based Sales Limits
Sales limits offer another policy tool with the potential to reduce excessive use and prevent harmful consumption. Sales limits, which restrict the amount of cannabis that a retailer can sell to an individual in a single transaction or over a period of time, have the added potential benefit of reducing diversion from the legal market. In comparison to potency limits, sales limits have been more widely implemented across states with recreational cannabis laws. Unfortunately, however, current state sales limits focus predominantly on product weight and cannabis type, not quantity of THC contained in each. As shown in Figure 3A, these limits vary considerably for concentrates.
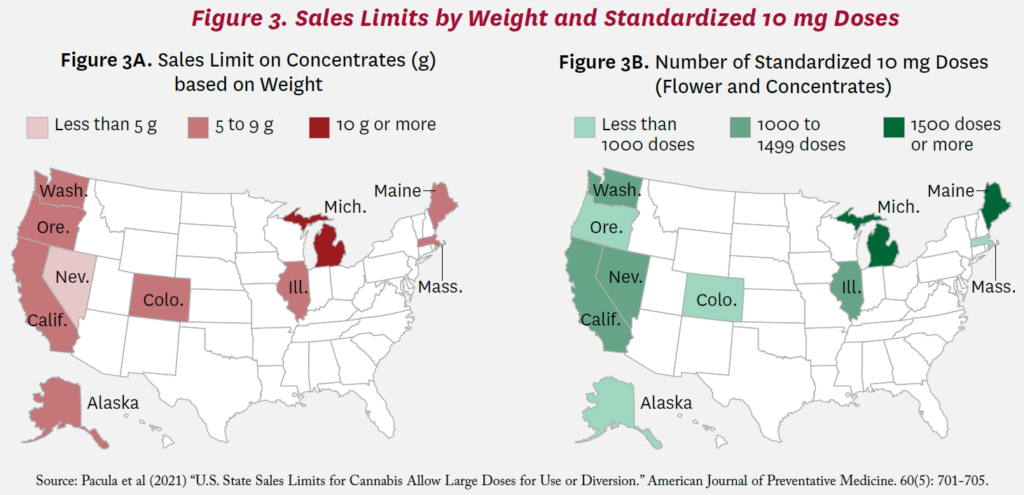
As of January 1, 2020, state weight-based sales limits ranged from 1 to 2.5 ounces for flower and 3.5 to 15 grams for concentrates.67 However, given differences in potency across products, a single transaction with the same weight of cannabis could represent substantially different amounts of total THC sold. At the lowest product potencies, the number of 10 milligram doses per transaction allowed under state laws ranged from 226 in Massachusetts to 1,046 in Michigan. Limits for average potency products exceeded 500 doses for every state and six states allowed single purchases exceeding 1,000 doses (Figure 3B).67 These sales limits allow large supplies for even individuals who use daily; with an average consumption of approximately 1.6 grams of flower per day, those who use daily could theoretically purchase more than a two-week supply in a single transaction.68,69
The July 2021 draft of the Senate proposal to legalize cannabis, the Cannabis Administration and Opportunity Act (CAOA), includes a retail sales limit even higher than current state policies, suggesting a retail sales limit of no more than 10 ounces of cannabis or the equivalent amount of any cannabis derivative in a single transaction.3 The stated intended purpose of this provision is to prevent diversion to the illegal market, but as Pacula et al. show, these limits are unlikely to accomplish this goal.67 Policymakers may also consider restricting the number of outlets a consumer can purchase from in a specified time period to better prevent diversion, which could be monitored and enforced through a retail sales system that tracks purchases by individual, not unlike a state prescription drug-monitoring program that tracks medications.67 Sales limits based on product weight alone also do little to discourage harmful cannabis consumption, as consumers can simply purchase products with higher potency.67
Other countries have effectively instituted much more restrictive sales limits than the U.S. In Uruguay, the sales limit for cannabis sold through pharmacies is 40 grams per month or 10 grams per week.55 Rather than placing limits on a single transaction, Uruguay is able to limit purchases over a period of time (per week and month) because each individual must be officially registered. This type of sales limit can better prevent excessive consumption as well as diversion, and was also implemented as part of several state medical cannabis laws here in the U.S. (e.g., Arizona). In the Netherlands, cannabis is not formally legalized for production and sale, but nonmedical purchases by adults have been tolerated through the Dutch coffee-shop system, where the sale of small amounts of cannabis is permitted for personal consumption under stringent guidelines. Though originally set at 30 grams, the sales limit for cannabis purchased at these coffee shops has dropped to 5 grams in order to combat drug tourism and misuse; the sales limit is still set based on product weight instead of potency.70 The lower sales limits implemented by these countries align better with public health and diversion concerns.
3. Designing a Tax Structure Based on Potency
Cannabis taxation is primarily thought of as a mechanism to raise revenue and help fund administrative costs associated with regulating the new market and enforcing its rules. However, taxation has also frequently been used as a public health tool for other intoxicating substances, particularly alcohol and tobacco.71,72 In the case of alcohol, the U.S. taxes products based on the amount of ethanol (the primary intoxicant in alcoholic beverages) contained in the drink, thereby taxing consumers based on the potential impairment and long-term harm associated with drinking alcohol, not the amount of liquid consumed. Taxation of cannabis in a similar fashion, based on intoxicating potential, may reduce excessive consumption and harmful use in a similar manner, as research has shown that cannabis use is responsiveness to price.73,74,75
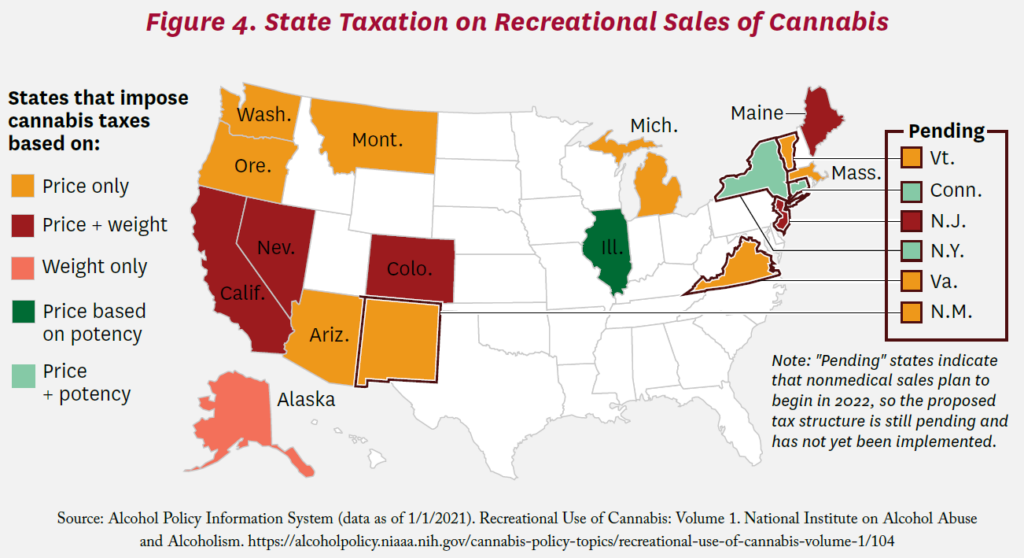
As shown in Figure 4, the majority of U.S. states with recreational cannabis laws have imposed retail-level, price-based taxes on cannabis products, ranging from 10% (in Michigan) to 37% (in Washington). While useful in mature markets where efficiencies in production have already been realized so prices of goods are relatively stable, price-based taxes do little to disincentivize consumption in emerging markets, particularly those with declining costs of production and growing competition. As mentioned previously, legalization of cannabis has led to a tremendous drop in the average price per gram of cannabis in Washington State due to gains in efficiency that occur with legalization. In Washington, retail prices per gram of flower declined by more than 50% between July 2014 and June 2017.15,76 Retail prices in Colorado have similarly declined, as the average price per THC dose for flower and concentrates in December 2020 was one-third of the price when recreational markets opened in 2014.16 When prices of goods fall by such substantial amounts, even large taxes do little to deter consumption. Moreover, tax revenue from price-based taxes will fall as prices fall, unless quantities purchased rise by a greater amount than the decline in prices, which contradicts the public health goal of preventing excessive consumption. Finally, large price-based taxes can incentivize consumers to seek out products with higher levels of THC so that consumers get more intoxicating effects per dollar spent. Washington State may exemplify this phenomenon—the state imposes a very high 37% retail price tax, and studies show a shift toward high-potency products (though this shift is not proven to be caused by the retail price tax).15 Thus, price-based taxes may not be an effective tool for accomplishing public health objectives, even if they generate revenue.
Some states, such as Alaska, California, Colorado, Maine and New Jersey, also impose taxes based on the weight of raw cannabis, which varies by type (e.g., flowers, leaves; see Figure 4). These taxes are similar to those on packs of cigarettes. Weight-based taxes do not lead to reduced tax revenue with declines in price but they too can incentivize producers to provide higher levels of THC per ounce.77
Only taxes based on the potency of cannabis products will provide the correct market incentives for both consumers and producers to moderate consumption. Taxes based on potency can disincentivize producers from generating high-potency products that will be taxed at a higher rate and disincentivize consumers from purchasing these products.18,78 Since a potency tax is not necessarily tied to price, tax revenue would remain more stable as efficiencies in production continue to emerge with federal legalization. As explained earlier, many states tax alcohol similarly, according to the percentage of a product’s volume that is ethanol.79 As of January 2021, Illinois is the only state that considers potency as part of its tax structure; it does not, however, institute a true tax based on potency, but rather a tax based on price and involving potency thresholds. Illinois’ unique system taxes “smokable” products (flower, vaping cartridges, dabs, etc.) with 35% THC or less at a rate of 10%, and those with more than 35% THC at a rate of 25%. However, “non-smokable” products (edibles, beverages, tinctures, etc.) are taxed at a rate of 20% regardless of their THC content. Connecticut (at the retail level) and New York (at the distribution level) are the only states that currently have plans to tax products based on potency; however, these taxes have not been implemented at the time of this writing. The states’ plans also include different THC tax rates depending on the product. The California Legislative Analyst’s Office also recommended a potency tax in a March 2022 report.80 Federally, the July 2021 draft of the CAOA does include a tax on potency, but only for extracts, and it begins five years after federal legalization occurs. This measure may be severely limited in its ability to protect public health. Experiences with the regulation of alcohol and tobacco exemplify that, even in the short-term, access to high-potency products may lead to increases in frequency of use.18 Moreover, the Washington State Liquor and Cannabis Board recently studied the feasibility of changing from an excise to a potency tax and concluded that a potency tax “could be a value for states that had not yet legalized or implemented their tax framework, but would present a costly infrastructure change to a state like ours that has,” suggesting the need for policymakers to carefully consider this policy tool more completely in the initial development of the tax structure.81
In comparison to potency caps and sales limits, taxing potency is a less utilized policy tool in Canada and Uruguay. In Canada, only oils, edibles, extracts and topicals are taxed at $0.01 per milligram of total THC.60 However, as noted previously, Canada places restrictions on grams of THC sold in a single transaction. In order to focus on eliminating the illegal market, Uruguay has implemented a variable fee instead of a fixed tax rate.82,83 Uruguay, however, utilizes both potency caps and sales limits to prevent excessive consumption.
4. Implementing Seed-to-Sale Data-Tracking Systems
Seed-to-sale tracking systems allow regulatory agencies to view every gram of legal cannabis throughout the supply chain. State and local governments use these systems to assist with enforcing regulations, collecting taxes, verifying product quality and preventing illegal cannabis diversion. Seed-to-sale tracking emerged from the medical software industry.84 The technology was originally developed as a prescription drug precursor tracking system to assist state government and law enforcement agencies in preventing drug diversion and promoting public safety. These systems can also be used to understand consumer product choice, allowing regulators to modify policies so as to moderate consumption.
To understand the impact that a heterogenous product like cannabis has on public health, it is important to understand which specific products are being consumed in terms of cannabinoid levels and mode of administration. Seed-to-sale tracking systems in Washington and Oregon have already demonstrated the value of collecting such information, identifying which products with high and low THC levels are gaining or losing market share in sales over time.13,15 Without FDA product regulation in place, these state seed-to-sale tracking systems have been the best source of data for researchers to gain insight into the actual potency of products being used; however, many states do not make this information readily available to outside researchers.
Seed-to-sale tracking systems permit comprehensive monitoring of product purchase behaviors and sales, surveillance of high-potency cannabis products through the legal supply chain, enforcement of potency caps, collection of taxes, and prevention of product diversion to youth or illegal markets. The systems can also enable quick recall of products if additives or other impurities are found. In addition to tracking all product concentration levels of CBD (a non-psychoactive component of cannabis), THC and other cannabinoids, platforms could also track pricing (including taxes) to facilitate evaluation of price responsivity of consumers to different products and identify whether some products should incur heavier taxes due to higher social costs.
All U.S. states with recreational cannabis laws require or plan to require some form of seed-to-sale tracking system, although implementation differs by state. A key limitation of many existing seed-to-sale platforms across states is the absence of information on customers. States may want to consider collecting information on the consumer to provide data for future regulations or assist with enforcement, such as enforcing limits on purchases within a day, week or month, as other countries do and as the U.S. does for medications that can be misused. Such regulations have been
implemented within regulated medical markets in some U.S. states. New York’s medical regulatory system requires detailed tracking of product characteristics (e.g., product type, potency levels) and administrative functions (e.g., prices, taxes), in addition to person-level characteristics (e.g., age and sex of the registered patient).85 Combining these detailed pieces of information, and examining individuals’ purchasing behaviors over time, is of great interest to public health because it can allow for targeted policy responses to curb excessive consumption of particular products rather than all cannabis-based products.
As legal cannabis markets open, tracking key transaction information is important for public health, particularly given the restrictions that have been in place on scientific inquiry of these products. To the extent that states can allocate resources toward using these databases for public health research or providing de-identified datasets to the broader research community, we can gain better insights regarding nuanced patterns of cannabis and cannabinoid consumption, behavioral changes in response to policy variation, and implications for health benefits or harms. Indeed, by making their seed-to-sale data publicly available, Washington State has been the subject of a wide number of studies that have advanced our understanding of product and price trends in legal cannabis markets, potential regulatory noncompliance by testing facilities, the extent to which legal cannabis markets crowd out illegal markets, and cross-product and cross-border shopping.15,40,68,69,86,88,89
Discussion
Our knowledge of the public health impacts of nonmedical, adult-use cannabis markets in U.S. states, Canada and Uruguay is still evolving. Gaps in knowledge may widen as legal cannabis markets’ product innovation outpaces the speed of scientific research. Just as we begin studies evaluating the impact of 5 or 10 milligram doses of THC, the cannabis industry produces a new product with far more THC in a single serving, delivering it in a candy bar, ice cream or other normalized product. Moreover, there are hundreds of combinations of cannabinoids in the plant and its derived products that might differentially influence health, but for which we have limited or no data.90 Additionally, though critically important in ascertaining the full impact of nonmedical, adult-use cannabis laws on health, the impact of cannabis use on alcohol and other substance use remains inconclusive.19,91
Despite these limitations, as the nation continues to move toward the liberalization of cannabis policies, policymakers should make the protection of public health an important goal. As outlined above, existing state laws and federal proposals thus far have largely failed to include policies that comprehensively promote reasonable cannabis use despite calls from international groups to do so.92,93 Resentencing, expungement of criminal records and dedicated funds to support organizations serving communities targeted by drug prohibition are all policies that should positively influence health outcomes and are included in federal proposals. However, policies to mitigate the harmful effects of high-potency products packaged as snacks and candies have received less consideration.
Regulations such as potency caps, time-based sales limits, taxes based on potency and a seed-to-sale tracking system that monitors sales of all cannabis-based products can provide boundaries that limit the promotion of harmful cannabis use by a profit-seeking cannabis industry. Research showing the harms of high-potency cannabis products and excessive use is emerging. Federal legalization proposals should seek to design a system promoting responsible use until the science around the products being generated from this plant is more fully understood.
References
- Gallup. (2021). Support for Legal Marijuana Holds at Record High of 68%. https://news.gallup.com/poll/356939/support-legal-marijuana-holds-record-high.aspx.
- 2021-2022 Marijuana Opportunity Reinvestment and Expungement Act. https://www.congress.gov/bill/117th-congress/house-bill/3617.
- Booker, C., R. Wyden and C. Schumer. (2021). Cannabis Administration & Opportunity Act. https://www.democrats.senate.gov/imo/media/doc/CAOA%20Detailed%20Summary%20-.pdf.
- Shi, Y., and R. L. Pacula. (2021). Assessment of Recreational Cannabis Dispensaries’ Compliance With Underage Access and Marketing Restrictions in California. JAMA Pediatrics, 175 (11): 1178-80.
- Wang, G. S., M.-C. Le Lait, S. J. Deakyne, A. C. Bronstein, L. Bajaj and G. Roosevelt. (2016). Unintentional Pediatric Exposures to Marijuana in Colorado, 2009-2015. JAMA Pediatrics, 170 (9): e160971.
- Shi, Y., and D. Liang. (2020). The Association Between Recreational Cannabis Commercialization and Cannabis Exposures Reported to the US National Poison Data System. Addiction, 115 (10): 1890-99.
- Whitehill, J. M., Dilley, J. A., Brooks-Russell, A., Terpak, L., & Graves, J. M. (2021). Edible Cannabis Exposures Among Children: 2017-2019. Pediatrics, 147(4). https://doi.org/10.1542/peds.2020-019893.
- Di Forti, M., D. Quattrone, T. P. Freeman et al. (2019). The Contribution of Cannabis Use to Variation in the Incidence of Psychotic Disorder Across Europe (EU-GEI): A Multicentre Case-Control Study. Lancet Psychiatry, 6 (5): 427-36.
- Freeman, T. P., and A. R. Winstock. (2015). Examining the Profile of High-Potency Cannabis and Its Association With Severity of Cannabis Dependence. Psychol Med, 45 (15): 3181-89.
- Preuss, U. W., M. A. Huestis, M. Schneider et al. (2021). Cannabis Use and Car Crashes: A Review. Frontiers in Psychiatry, 12 (May): 643315.
- Kilmer, B., and R. L. Pacula. (2017). Building the Data Infrastructure to Evaluate Cannabis Legalization. Addiction, 112 (7): 1140-41.
- Vergara, D., L. C. Bidwell, R. Gaudino et al. (2017). Compromised External Validity: Federally Produced Cannabis Does Not Reflect Legal Markets. Scientific Reports, 7 (Apr.): 46528.
- Firth, C. L., S. Davenport, R. Smart and J. A. Dilley. (2020). How High: Differences in the Developments of Cannabis Markets in Two Legalized States. International Journal of Drug Policy, 75 (Jan.): 102611.
- Sevigny, E. L., R. L. Pacula and P. Heaton. (2014). The Effects of Medical Marijuana Laws on Potency. International Journal of Drug Policy, 25 (2): 308-19.
- Smart, R., J. P. Caulkins, B. Kilmer, S. Davenport and G. Midgette. (2017). Variation in Cannabis Potency and Prices in a Newly Legal Market: Evidence from 30 Million Cannabis Sales in Washington State. Addiction, 112 (12): 2167-77.
- MPG Consulting and Leeds School of Business. (2020). Regulated Marijuana Market Update. Colorado Department of Revenue, Marijuana Enforcement Division. https://sbg.colorado.gov/sites/sbg/files/2020-Regulated-Marijuana-Market-Update-Final.pdf.
- Cerda, M., C. Mauro, A. Hamilton, N. S. Levy, J. Santaella-Tenorio, D. Hasin, M. M. Wall, K. M. Keyes and S. S. Martins. (2020). Association Between Recreational Marijuana Legalization in the United States and Changes in Marijuana Use and Cannabis Use Disorder From 2008 to 2016. JAMA Psychiatry, 77 (2): 165-71.
- Hall, W., and M. Lynskey. (2020). Assessing the Public Health Impacts of Legalizing Recreational Cannabis Use: The US Experience. World Psychiatry, 19 (2): 179-86.
- Smart, R., and R. L. Pacula. (2019). Early Evidence of the Impact of Cannabis Legalization on Cannabis Use, Cannabis Use Disorder, and the Use of Other Substances: Findings From State Policy Evaluations. American Journal of Drug and Alcohol Abuse, 45 (6); 644-63.
- Volkow, N. D., B. Han, W. M. Compton and E. F. McCance-Katz. (2019). Self-Reported Medical and Nonmedical Cannabis Use Among Pregnant Women in the United States. JAMA, 322 (2): 167-69.
- Wang, G. S., C. Buttorff, A. Wilks, D. Schwam, T. D. Metz, G. Tung and R. L. Pacula. (2022). Cannabis Legalization and Cannabis-Involved Pregnancy Hospitalizations in Colorado. Preventive Medicine, 156 (Mar.): 106993.
- Young-Wolff, K. C., V. Sarovar, L.-Y. Tucker, A. Conway, S. Alexeeff, C. Weisner, M. A. Armstrong and N. Goler. (2019). Self-Reported Daily, Weekly, and Monthly Cannabis Use Among Women Before and During Pregnancy. JAMA Network Open, 2 (7): e196471.
- Richards, J. R., N. E. Smith and A. K. Moulin. (2017). Unintentional Cannabis Ingestion in Children: A Systematic Review. Journal of Pediatrics, 190 (Nov.): 142-52
- Roehler, D. R., B. E. Hoots, K. M. Holland, G. T. Baldwin and A. M. Vivolo-Kantor. (2022). Trends and Characteristics of Cannabis-Associated Emergency Department Visits in the United States, 2006-2018. Drug and Alcohol Dependance, 232 (Mar.): 109288.
- Wang, G. S., S. D. Davies, L. S. Halmo, A. Sass and R. D. Mistry. (2018). Impact of Marijuana Legalization in Colorado on Adolescent Emergency and Urgent Care Visits. Journal of Adolescent Health, 63 (2): 239-41.
- Hartman, R. L., and M. A. Huestis. (2013). Cannabis Effects on Driving Skills. Clinical Chemistry, 59 (3): 478-92.
- Kamer, R. S., S. Warshafsky and G. C. Kamer. (2020). Change in Traffic Fatality Rates in the First 4 States to Legalize Recreational Marijuana. JAMA Internal Medicine, 180 (8): 1119-20.
- Lira, M. C., T. C. Heeren, M. Buczek, J. G. Blanchette, R. Smart, R. L. Pacula and T. S. Naimi. (2021). Trends in Cannabis Involvement and Risk of Alcohol Involvement in Motor Vehicle Crash Fatalities in the United States, 2000-2018. American Journal of Public Health, 111 (11): 1976-85.
- Vingilis, E., J. S. Seeley, P. Di Ciano et al. (2021). Systematic Review of the Effects of Cannabis Retail Outlets on Traffic Collisions, Fatalities and Other Traffic-Related Outcomes. Journal of Transport & Health, 22 (Sep.): 101123.
- Chandra, S., M. M. Radwan, C. G. Majumdar, J. C. Church, T. P. Freeman and M. A. ElSohly (2019). New Trends in Cannabis Potency in USA and Europe During the Last Decade (2008–2017). European Archives of Psychiatry and Clinical Neuroscience, 269 (1): 5-15.
- Wadsworth, E., and D. Hammond. (2019). International Differences in Patterns of Cannabis Use Among Youth: Prevalence, Perceptions of Harm, and Driving Under the Influence in Canada, England & United States. Addictive Behaviors, 90 (Mar.), 171-75.
- Spindle, T. R., M. O. Bonn-Miller and R. Vandrey. (2019). Changing Landscape of Cannabis: Novel Products, Formulations, and Methods of Administration. Current Opinion in Psychology, 30 (Dec.): 98-102;
- Volkow, N. D., & Weiss, S. R. B. (2020). Importance of a standard unit dose for cannabis research. Addiction, 115(7), 1219-1221. https://doi.org/10.1111/add.14984.
- Committee on the Health Effects of Marijuana, Board on Population Health and Public Health Practice, Health and Medicine Division. (2017). The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press.
- Colizzi, M., M. Ruggeri and S. Bhattacharyya. (2020). Unraveling the Intoxicating and Therapeutic Effects of Cannabis Ingredients on Psychosis and Cognition. Frontiers in Psychology, 11 (May 14).
- Volkow, N. D., J. M. Swanson, A. E. Evins et al. (2016). Effects of Cannabis Use on Human Behavior, Including Cognition, Motivation, and Psychosis: A Review. JAMA Psychiatry, 73 (3): 292-97.
- Hall, W. (2015). What Has Research Over the Past Two Decades Revealed About the Adverse Health Effects of Recreational Cannabis Use? Addiction, 110 (1): 19-35.
- Dilley, J. A., J. M. Graves, A. Brooks-Russell, J. M. Whitehill and E. L. Liebelt. (2021). Trends and Characteristics of Manufactured Cannabis Product and Cannabis Plant Product Exposures Reported to US Poison Control Centers, 2017-2019. JAMA Network Open, 4 (5): e2110925.
- Myran, D. T., N. Cantor, Y. Finkelstein, M. Pugliese, A. Guttmann, R. Jesseman and P. Tanuseputro. (2022). Unintentional Pediatric Cannabis Exposures After Legalization of Recreational Cannabis in Canada. JAMA Network Open, 5 (1): e2142521.
- Davenport, S. (2021). Price and Product Variation in Washington’s Recreational Cannabis Market. International Journal of Drug Policy, 91 (May): 102547.
- Wang, G. S., C. Buttorff, A. Wilks, D. Schwam, G. Tung and R. L. Pacula. (2021). Changes in Emergency Department Encounters for Vomiting After Cannabis Legalization in Colorado. JAMA Network Open, 4 (9): e2125063.
- Wang, G. S., C. Buttorff, A. Wilks, D. Schwam, G. Tung and R. L. Pacula. (2022). Impact of Cannabis Legalization on Healthcare Utilization for Psychosis and Schizophrenia in Colorado. International Journal of Drug Policy, 104 (Jun): 103685.
- ElSohly, M. A., Chandra, S., Radwan, M., Majumdar, C. G., & Church, J. C. (2021). A comprehensive review of cannabis potency in the United States in the last decade. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 6(6), 603-606.
- Mehmedic, Z., Chandra, S., Slade, D., Denham, H., Foster, S., Patel, A. S., … & ElSohly, M. A. (2010). Potency trends of Δ9‐THC and other cannabinoids in confiscated cannabis preparations from 1993 to 2008. Journal of Forensic Sciences, 55(5), 1209-1217.
- Cash, M. C., K. Cunnane, C. Fan and E. A. Romero-Sandoval. (2020). Mapping Cannabis Potency in Medical and Recreational Programs in the United States. PloS One, 15 (3): e0230167.
- Boakye, E., O. H. Obisesan, S. M. I. Uddin et al. (2021). Cannabis Vaping Among Adults in the United States: Prevalence, Trends, and Association with High-Risk Behaviors and Adverse Respiratory Conditions. Preventive Medicine, 153 (Dec.).
- Goodman, S., E. Wadsworth, C. Leos-Toro, D. Hammond and International Cannabis Policy Study Team. (2020). Prevalence and Forms of Cannabis Use in Legal vs. Illegal Recreational Cannabis Markets. International Journal of Drug Policy, 76 (Feb.): 102658.
- Wadsworth, E., C. Leos-Toro and D. Hammond. (2020). Mental Health and Medical Cannabis Use Among Youth and Young Adults in Canada. Substance Use & Misuse, 55 (4): 582-89.
- Vermont General Assembly. (2020). No. 164. An Act Relating to the Regulation of Cannabis. https://legislature.vermont.gov/Documents/2020/Docs/ACTS/ACT164/ACT164%20As%20Enacted.pdf.
- Connecticut General Assembly (2022). Sec. 21a-421j 14, Chapter 420h – REGULATION OF ADULT-Use Cannabis (ct.gov) https://www.cga.ct.gov/2022/sup/chap_420h.htm
- Schroyer, J. (2021). Marijuana Foes Seek to Impose THC Potency Caps to Curb Industry’s Growth. MJBiz Daily, January 25. https://mjbizdaily.com/marijuana-foes-seekto-impose-thc-potency-caps-to-curb-industrys-growth.
- Burness, A. (2021). Colorado May See Its Biggest Overhaul of Marijuana Laws Since Recreational Legalization. The Denver Post, March 11. https://www.denverpost.com/2021/03/11/colorado-biggest-overhaul-marijuana-laws-thc-cap.
- Morgan, I. (2021). Tweets and Emails Helped Kill a FL Bill to Place a Cap on High-Potency Medical Marijuana for Patients. Florida Phoenix, May 6. https://floridaphoenix.com/2021/05/06/tweets-and-emails-helped-kill-a-fl-bill-to-place-a-capon-high-potency-medical-marijuana-for-patients.
- Schuba, T. (2022, January 25, 2022). Bill to limit THC in pot sold at dispensaries draws swift backlash: ‘It’s almost impossible’. Retrieved April 15 from https://chicago.suntimes.com/cannabis/2022/1/25/22901763/illinois-dispensaries-pot-cannabis-thc-limits-legislaturemedical-society-posion-control-edible.
- United Nations Office on Drugs and Crime. (2021). Drug Market Trends: Cannabis, Opioids. World Drug Report 2021. https://www.unodc.org/res/wdr2021/field/WDR21_Booklet_3.pdf.
- Pardal, M., R. Queirolo, E. Álvarez and L. Repetto. (2019). Uruguayan Cannabis Social Clubs: From Activism to Dispensaries? International Journal of Drug Policy, 73 (Nov.) 49-57.
- European Monitoring Centre for Drugs and Drug Addiction. (2018). Uruguay Reports on Regulated Cannabis Growing and Sales. https://www.emcdda.europa.eu/news/2018/uruguay-reports-on-regulatedcannabis-growing-and-sales_en.
- Government of Canada (2022). Final Regulations: Edible Cannabis, Cannabis Extracts, Cannabis Topicals. https://www.canada.ca/content/dam/hc-sc/documents/services/drugs-medication/cannabis/resources/finalregulationsedible-cannabis-extracts-topical-eng.pdf.
- Naimi, T. S., K. Vallance, S. Churchill, R. Callaghan, T. Stockwell and A. Farrell-Low. (2021). Sales and Revenue from Regulated Cannabis Products: British Columbia, October 2018–December 2020. University of Victoria, Canadian Institute for Substance Use Research. https://www.uvic.ca/research/centres/cisur/assets/docs/reportsales-and-revenue-from-regulated-cannabis-products-bc.pdf.
- Pacula, R. L., R. Jesseman and R. N. Bluthenthal. (2021). Regulating Cannabis for Public Health. Schaeffer Center for Health Policy & Economics, Institute for Addiction Sciences. https://healthpolicy.usc.edu/events/regulating-cannabis-for-public-health.
- Drug Enforcement Administration. Implementation of the Agriculture Improvement Act of 2018. (2020). https://www.deadiversion.usdoj.gov/fed_regs/rules/2020/.fr0821.htm.
- Food and Drug Administration (2022). 5 Things to Know About Delta-8 Tetrahydrocannabinol–Delta-8 THC. March 18. https://www.fda.gov/consumers/consumer-updates/5-things-know-about-delta-8-tetrahydrocannabinol-delta-8-thc.
- Schauer, G. (2021). Delta-8 THC and other THC Analogues: Health and Consumer Safety Considerations. Presentation to the Washington State House Commerce & Gaming Committee, October 21. https://app.leg.wa.gov/committeeschedules/Home/Document/236368.
- Willner, N. (2022). The Controlled Substances Act Leaves Pathway for Intoxicating Hemp-Derived Cannabinoids. MJBiz Daily, Feb. 1. https://mjbizdaily.com/the-controlled-substances-act-leaves-pathway-forintoxicating-hemp-derived-cannabinoids.
- Quttaineh, R. (2021). Future of Delta 8 Products Unclear in ND as Legislators Amend Hemp Regulations. KVRR Local News, April 22. https://www.kvrr.com/2021/04/22/future-of-delta-8-products-unclear-in-nd-as-legislatorsamend-hemp-regulations.
- Staff, M. (2021). Michigan Governor Moves to Regulate Delta-8 THC Products. MJBiz Daily, December 17. https://mjbizdaily.com/michigan-governor-moves-toregulate-delta-8-thc-products/#:~:text=Michigan%20Gov.,sold%20in%20unlicensed%20retail%20stores.
- Pacula, R. L., J. G. Blanchette, M. C. Lira, R. Smart and T. S. Naimi. (2021). Current U.S. State Cannabis Sales Limits Allow Large Doses for Use or Diversion. American Journal of Preventive Medicine, 60 (5): 701-5.
- Caulkins, J. P., S. Davenport, A. Doanvo, K. Furlong, A. Siddique, M. Turner and B. Kilmer. (2019). Triangulating Web and General Population Surveys: Do Results Match Legal Cannabis Market Sales? International Journal of Drug Policy, 73: 293-300.
- Kilmer, B., S. Davenport, R. Smart, J. P. Caulkins and G. Midgette. (2019). After the Grand Opening: Assessing Cannabis Supply and Demand in Washington State. RAND Corporation. https://www.rand.org/pubs/research_reports/RR3138.html.
- Caulkins, J. P., and B. Kilmer. (2016). Considering Marijuana Legalization Carefully: Insights for Other Jurisdictions from Analysis for Vermont. Addiction, 111 (12): 2082-89.
- Chaloupka, F. J., A. Yurekli and G. T. Fong. (2012). Tobacco Taxes as a Tobacco Control Strategy. Tobacco Control, 21 (2): 172-80.
- Cook, P. J. (2007). Paying the Tab: The Costs and Benefits of Alcohol Control. Princeton: Princeton University Press.
- Hall, W., and R. L. Pacula. (2003). Cannabis Use and Dependence: Public Health and Public Policy. Cambridge: Cambridge University Press.
- Pacula, R. L., M. Grossman, F. J. Chaloupka, P. M. O’Malley, L. D. Johnston and M. C. Farrelly. (2001). Marijuana and Youth. In Risky Behavior Among Youths: An Economic Analysis, edited by J. Gruber, 271-326. Chicago: University of Chicago Press.
- Pacula, R. L., and R. Lundberg. (2014). Why Changes in Price Matter When Thinking About Marijuana Policy: A Review of the Literature on the Elasticity of Demand. Public Health Review, 35 (2): 1-18.
- Hansen, B., K. Miller, B. Seo and C. Weber. (2020). Taxing the Potency of Sin Goods: Evidence From Recreational Cannabis and Liquor Markets. National Tax Journal, 73 (2): 511-44.
- Shover, C. L., and K. Humphreys. (2019). Six Policy Lessons Relevant to Cannabis Legalization. American Journal of Drug and Alcohol Abuse, 45 (6): 698-706. https://doi.org/10.1080/00952990.2019.1569669.
- Caulkins, J. P., B. Kilmer, M. A. R. Kleiman, R. J. MacCoun, G. Midgette, P. Oglesby, R. L. Pacula and P. Reuter. (2015). Considering Marijuana Legalization: Insights for Vermont and Other Jurisdictions. RAND Corporation, RR-864.
- Alcohol Policy Information System. (2022). Alcohol Beverages Taxes. https://alcoholpolicy.niaaa.nih.gov.
- California Legislative Analyst’s Office. (2022). California’s Cannabis Taxes. March 1. https://lao.ca.gov/handouts/state_admin/2022/California%E2%80%99s-Cannabis-Taxes-030122.pdf.
- Washington State Liquor and Cannabis Board. (2019). Taxing Cannabis by Potency: A Feasibility Study. Legislative Directed Work Group Report. https://lcb.wa.gov/sites/default/files/publications/Marijuana/Potency_Tax_Study/Cannabis-Potency-Tax-Workgroup_Report_FINAL.PDF.
- Hansen, B., K. Miller and C. Weber. (2021). Up in Smoke? The Market for Cannabis. In Handbook of Labor, Human Resources and Population Economics, edited by K. F. Zimmerman. New York: Springer Reference.
- Walsh, J., and G. Ramsey. (2015). Uruguay’s Drug Policy: Major Innovations, Major Challenges. Foreign Policy at Brookings. https://www.brookings.edu/wp-content/uploads/2016/07/Walsh-Uruguay-final.pdf.
- 2017 Drug Supply Chain Security Act, https://www.fda.gov/drugs/drug-supply-chain-integrity/drug-supply-chain-security-act-dscsa.
- Kritikos, A. F. (2021). Dose of Reality: Who Are Medical Cannabis Patients? Essays on Purchasing Patterns and Alcohol Consumption Among Users in New York State. PhD diss., Brandeis University.
- Caulkins, J. P., Y. Bao, S. Davenport et al. (2018). Big Data on a Big New Market: Insights from Washington State’s
Legal Cannabis Market. International Journal of Drug Policy, 57: 86-94. - Jikomes, N., and M. Zoorob. (2018). The Cannabinoid Content of Legal Cannabis in Washington State Varies Systematically Across Testing Facilities and Popular Consumer Products. Scientific Reports, 8 (1): 4519.
- Hansen, B., K. Miller and C. Weber. (2020). Federalism, Partial Prohibition, and Cross-Border Sales: Evidence From Recreational Marijuana. Journal of Public Economics, 187 (Jul.): 104159.
- Miller, K., and B. Seo. (2021). The Effect of Cannabis Legalization on Substance Demand and Tax Revenues. National Tax Journal, 74 (1): 107-45.
- Boesen, U. (2020). “A Road Map to Recreational Marijuana Taxation.” Tax Foundation, No. 713. June 9. https://files.taxfoundation.org/20200608144852/A-Road-Map-to-Recreational-Marijuana-Taxation.pdf.
- Pacula, R. L., R. Smart, M. C. Lira, S. C. Pessar, J. G. Blanchette and T. S. Naimi. (2022). Relationships of Cannabis Policy Liberalization With Alcohol Use and Co-Use With Cannabis: A Narrative Review. Alcohol Research, 42 (1): 6.
- Fischer, B., T. Robinson, C. Bullen et al. (2022). Lower- Risk Cannabis Use Guidelines (LRCUG) for Reducing Health Harms from Non-medical Cannabis Use: A Comprehensive Evidence and Recommendations Update. International Journal of Drug Policy, 99 (Jan.): 103381.
- Fischer, B., C. Russell, P. Sabioni, W. van den Brink, B. Le Foll, W. Hall, J. Rehm and R. Room. (2017). Lower-Risk Cannabis Use Guidelines: A Comprehensive Update of Evidence and Recommendations. American Journal of Public Health, 107 (8): E1-12.
You must be logged in to post a comment.