What’s the latest in health policy research? The Essential Scan, produced by the Schaeffer Initiative for Innovation in Health Policy, aims to help keep you informed on the latest research and what it means for policymakers.
Hospital list prices not associated with quality but do increase payments for privately insured
Michael Batty and Benedic Ippolito find that over the period of 2002 to 2014, hospital characteristics such as size, for-profit status, location, and affiliation with a larger health system are the largest predictors of hospital list prices, also known as chargemaster rates, and that higher rates are positively associated with the amounts actually paid by the patients and their insurer. For example, a large, urban, for-profit hospital affiliated with a larger health system had list prices 360 percent more than those of a small, rural, independent hospital. Quality, however, was not positively associated with price, as the authors find no significant relationship between cost and quality after controlling for patient and disease characteristics. Payments made for care for privately insured patients increased 15 cents for every additional dollar in list price, while the impact on payments made for publicly insured patients was not statistically significant. These findings call into question the notion that chargemaster rates have little and decreasing impact on payments for care as more Americans receive coverage. Full article here.
Greater post-discharge pharmacy services may improve care for Medicaid managed care beneficiaries
Weiyi Ni, Danielle Colayco, Jonathan Hashimoto, and coauthors find that the use of a pharmacy-based transition of care program reduced hospital readmissions by 28 percent within 30 days of discharge and by 31.9 percent within 6 months of discharge among managed Medicaid beneficiaries compared to a control group of patients in the health system who were discharged from neighboring hospitals. This was the first study of it’s kind at a community pharmacy, adding to the body of literature finding that patients continue to benefit from pharmacy services beyond discharge. Full article here.
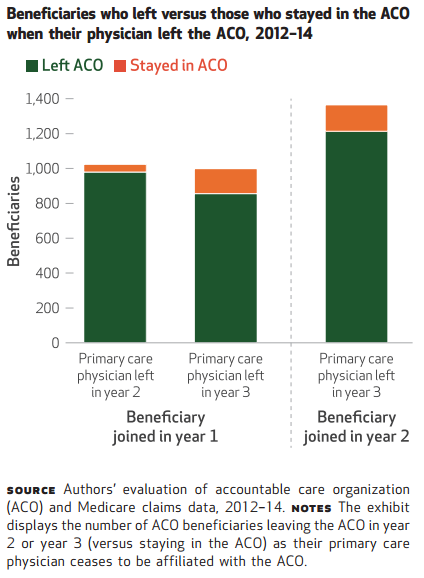
Medicare Pioneer ACO experienced significant churn of both physicians and beneficiaries, highlighting potential for contract gaming
John Hsu, Christine Vogeli, Mary Price, and coauthors find that 41 percent of physicians associated with an Accountable Care Organization (ACO) during the 2012 – 2014 contract period joined partway through the contract and 18 percent left. The authors found that this churn also affected beneficiaries’ affiliation, as 49 percent new-to-the-ACO beneficiaries became aligned because their physician joined the ACO, not because of a change of providers. Similarly, 90 percent of the beneficiaries attributed to a physician exiting the ACO also exited. The authors find that even smaller shares of physician churn than those observed create significant potential for “gaming” the ACO contract. For example, they find that if 5 percent of the primary care physicians with the highest cost attributed beneficiaries were dropped from ACO participation, the average per capita spending in an ACO would decrease 17 percent. These findings underscore the potential for gaming the system, as well as offer provider churn as a possible explanation for the early muted impact of ACOs on total cost. Full article here.
“This is an eye-opening study addressing an issue that has not been given much attention. It speaks to weaknesses in the ACO models used by Medicare.” – Paul Ginsburg, PhD, Director of the Schaeffer Initiative
ACA’s Medicaid expansion and private insurance reforms reduced cost-of-care barrier by 5.1 percentage points, personal health behaviors remain unaffected
Charles Courtemanche, James Marton, Benjamin Ukert, and co-authors find that the Affordable Care Act increased multiple dimensions of health care access through both its private insurance reforms and Medicaid expansion, with states that expanded Medicaid netting the greatest gains. For example, changes to the private individual market increased an individual’s likelihood of having insurance coverage, an established primary care doctor, and a well-patient checkup by 5.3, 3.0, and 2.4 percentage points, respectively. Combined private insurance and Medicaid expansion also was found to reduce the probability of cost being a barrier to treatment by 5.1 percentage points. However, neither Medicaid expansion nor private market reforms resulted in statistically significant impacts on self-assessed health status, body mass indices, probability of being a smoker, or number of drinks per month. These findings highlight the clear health care access gains associated with the full ACA implementation, while illustrating the complexity of linking health care access to changes in personal health behaviors. The findings from this study contrast with the improved health behaviors or self-assessed health status found in studies of state-based health expansions. Full article here.
Click here to receive The Essential Scan email.
Editor’s Note: The Essential Scan is produced by the Schaeffer Initiative for Innovation in Health Policy, a collaboration between the Center for Health Policy at the Brookings Institution and the USC Schaeffer Center for Health Policy & Economics. To receive the Essential Scan in your inbox, sign up here.