
Will clinicians become more careful in prescribing opioids if they are made of aware of the risks of these drugs first-hand? That was one of the core questions researchers set out to explore in a new study published in the August 2018 issue of Science. In doing so, they found that many clinicians do not learn of the deaths of those patients who overdose as they just disappear from their practice, outcomes unknown.
This disconnect from the personal experience of losing a patient due to fatal overdose, related to a prescription for opioids to relieve pain, makes the problem of the nation’s opioid crisis seem remote – statistics happening elsewhere. While the epidemic continues to exert its outsized impact, opioid prescription-writing levels have not responded with adequate risk-benefit analysis by prescribers tasked with caring for patients with complaints around pain.
“Clinicians may never know a patient they prescribed opioids to suffered a fatal overdose,” explained lead author Jason Doctor. “What we wanted to evaluate is whether closing that information gap will make them more judicious prescribers.” Doctor is the Director of Health Informatics at the USC Schaeffer Center for Health Policy & Economics and Associate Professor at the Price School of Public Policy.
Clinicians may never know a patient they prescribed opioids to suffered a fatal overdose.
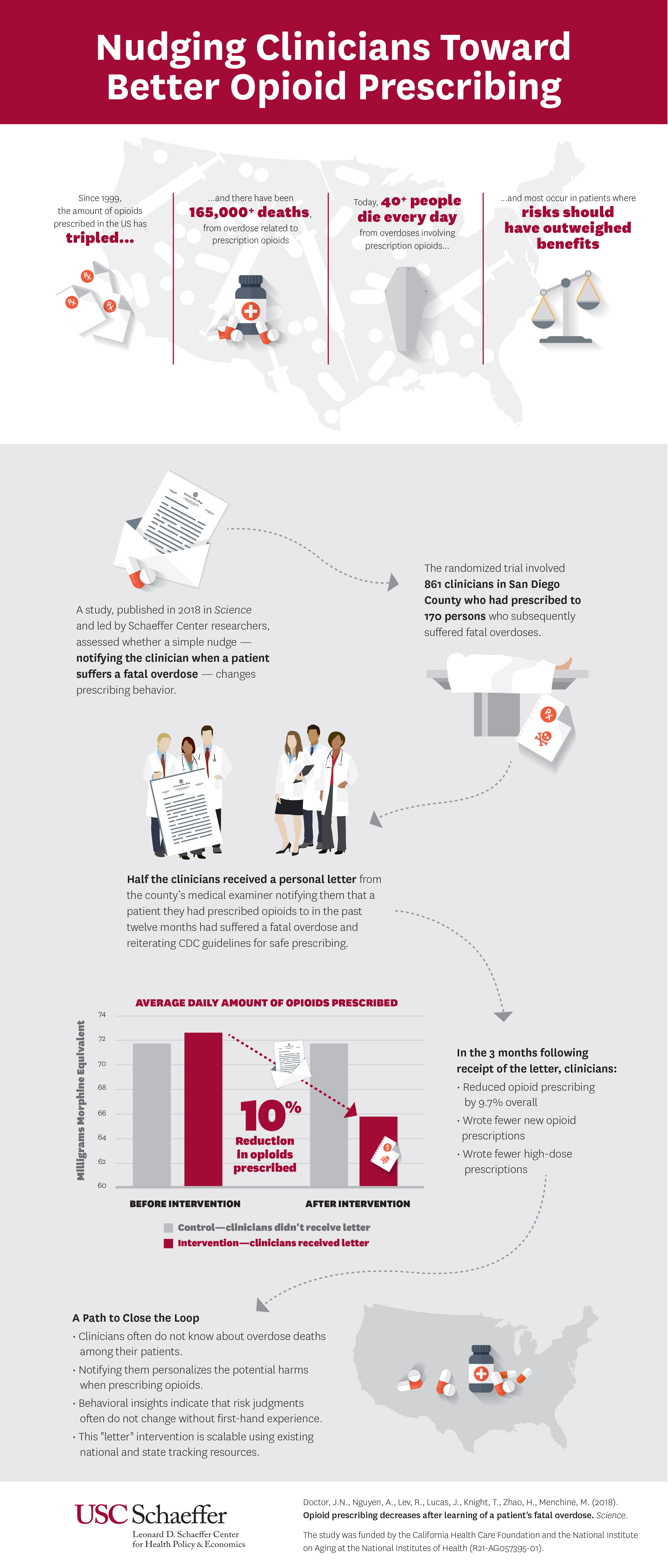
The study leverages behavioral insights and psychology to give prescribers personal experience with the risk associated with opioids, and finds that when a clinician learns one of their patients had suffered a fatal overdose they reduced the amount of opioids prescribed by almost 10 percent in the following three months.
Doctor and his colleagues conducted a randomized trial between July 2015 and June 2016 of 861 clinicians who had prescribed to 170 patients who subsequently suffered a fatal overdose involving prescription opioids. Half the clinicians, who all practiced in San Diego County, were randomly selected to receive a letter from the county medical examiner notifying them that a patient they had prescribed opioids to in the past twelve months had a fatal overdose. The letter, which was supportive in tone, also provided information from the Centers for Disease Control (CDC) on safe prescribing guidelines, nudging clinicians toward better prescribing habits.
In the three months after receiving the letter, prescribing decreased by 9.7 percent compared to the control group who didn’t receive a letter. Furthermore, clinicians who received the letter were 7 percent less likely to start a new patient on opioids and less likely to prescribe higher doses.
The results are particularly exciting given that numerous, more traditional state regulations which often involve mandated limits on opioids have not been shown to have much impact. The authors point to numerous reasons why this study showed more promising results including its simplicity, that the letters still allows clinicians to decide when they will prescribe opioid analgesics and that it provides an important missing piece of clinical information to them.
This intervention is easily scalable nationwide as existing state and national resources already track the information necessary around overdose deaths associated with prescription and illicit drugs.
“Interventions that use behavioral insights to nudge clinicians to correct course are powerful, low-cost tools because they maintain the autonomy of the physician to ultimately decide the best course of care for their patient,” said Doctor. “In this case, we know opioids, though beneficial to some patients with certain conditions, come with high risks that the doctor may not fully grasp when observing patients in the clinic. Providing information about harm that would otherwise go unseen by them gives physicians a clearer picture.”
Co-authors include Andy Nguyen, Roneet Lev, Jonathan Lucas, Tara Knight, Henu Zhao, and Michael Menchine. Funding for the study was provided by the California Health Care Foundation and the National Institute on Aging at the National Institutes of Health (R21-AG057395-01).
You must be logged in to post a comment.